

Seconds
Seconds

Audio Recording by George Hahn
We receive dozens of thoughtful emails each week from people (mostly young men) asking for advice. They all deserve a response, but the time/space continuum gets in the way. So we’ve set out to leverage AI to develop a digital twin capable of answering questions in my voice. ProfG.ai is an experiment we hope will provide insight into AI and (someday) help people make better decisions re their offline lives. Or not. For more about how and why we made it, check out our podcast announcement here.
—
Disrupted
Disruptive innovation is often felt more in second-order effects, clear of the original idea’s blast zone. The automobile was transformative, not because of the cars but the suburban lifestyle they inspired. Global power was increasingly shaped by the flow of energy. And the manufacturing innovation required to wrap steel around four wheels and an engine at scale became central to the West’s economy.
Today the media (including this newsletter) is obsessed with the changes wrought by artificial intelligence. In my view, it’s an obsession caused by the collision of techno-narcissism and the idolatry of innovators. Our new gods, tech innovators, posit that they are the fathers of the singular point of leverage that will save or destroy humanity. “Now that my options have vested, I want to profess that I am such a fucking genius, I’m now worried about my brilliance being unleashed. I’m so awesome as to be dangerous, accidentally of course.”
Jesus Christ, get over yourself.
I believe there is another innovation that will also be transformative as its full impact and second-order effects play out. What GPT is to the media, GLP-1 will be to the real economy.
GLP-1 > GPT 4
GLP-1 is an agonist, a hormone our bodies use for internal communication. Among other things, it triggers the pancreas to produce insulin, which brought it to the attention of diabetes researchers, who developed a synthetic form of GLP-1 called semaglutide. In 2017, Novo Nordisk brought semaglutide to market in the U.S., under the brand name Ozempic.
Note: My use of the word “agonist” in the previous paragraph was an attempt to appear more intellectually svelte. My use of the word “svelte” in the previous sentence is an attempt to sound prim. Using “prim,” more British. Trying, always trying … desperate for other people’s affirmation. But I digress.
The scientists who developed semaglutide faced a problem when conducting their research — if the dose was too high, patients taking the drug lost their appetite. Ozempic was formulated at a low enough dose to reduce this side effect. However, Novo Nordisk realized this was a feature, not a bug, and formulated a higher-dose class specifically for weight loss, Wegovy, approved in 2021.
Semaglutide will be followed by similar GLP-1 drugs, including retatrutide and tirzepatide, both in trials from Eli Lilly. Studies with overweight patients show weight loss of 15% to 24% of body weight. Both Wegovy and Ozempic are weekly injectables, which discourages some people, but now there’s a pill version, Rybelsus. Whatever the label on the box, GLP-1 drugs make us feel fuller for longer and suppress hunger cravings. In sum: the most effective weight loss drugs to-date.
Hungry Market
The market for this product, and the potential for meaningful societal change, are massive. In America, 70% of people are obese or overweight. There isn’t anything that over two-thirds of America is. (Only 30% of Americans watched the last season premiere of Game of Thrones.) More than 42% of U.S. adults are obese, up from 31% in 1991. Globally, the prevalence of obesity has tripled since 1975, and 800 million people, including 50 million children, are now obese. People with limited access to healthy food or bad genetic luck with their body chemistry are preyed upon by one of the most well-oiled marketing and distribution engines ever built: the industrial food complex. They’d like to teach the world to sing, in perfect harmony with addiction and diabetes.
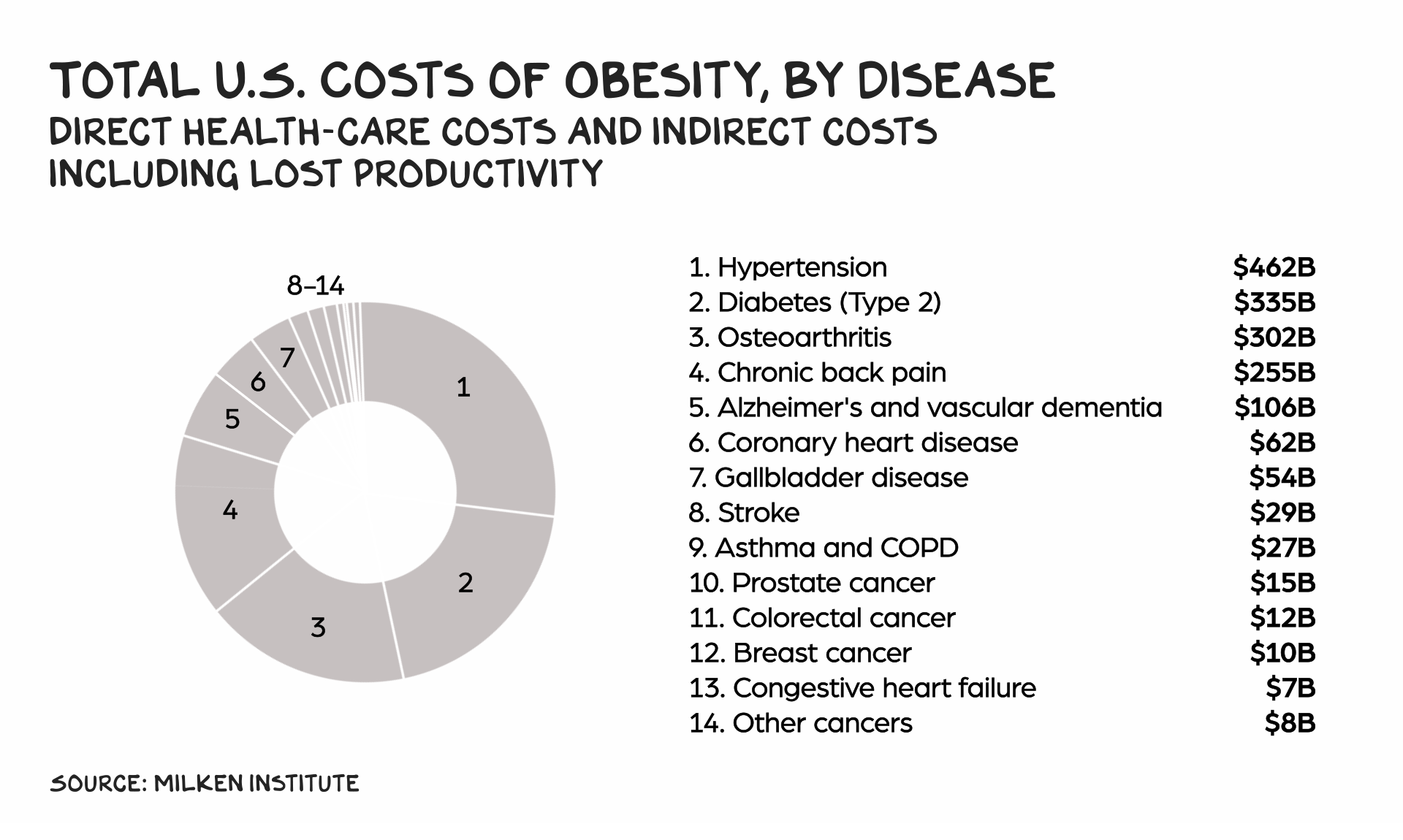
Obesity is not a form of personal expression or finding one’s “truth,” it’s a disease that invites illness and disability, including coronary heart disease, stroke, cancer, gallbladder disease, and Type 2 diabetes. Globally, obesity is the fifth-largest cause of premature death. Our health-care system suffers from many problems, and the chaser to many/most of them is obesity. According to The Milken Institute the direct and indirect costs of obesity total $1.7 trillion, or 7% of U.S. GDP. A 15% reduction in body weight would move 43 million Americans out of the obese column.
In the fourth quarter of 2022, 9 million prescriptions for GLP-1 drugs were written in the U.S. Over the past two years the share of health-care patients in the U.S. using semaglutide has tripled to 1.7%. That number will grow, as an estimated 93 million Americans could benefit from the drug. I believe even that understates the economic opportunity for Novo Nordisk (and, eventually, other GLP-1 drugmakers), as the numbers understate the demand. In the past 24 hours I have spoken to three people, whom I wouldn’t describe as being overweight, much less obese, who are on Ozempic to lose that last stubborn 15 pounds.

What happens when millions of people start taking a drug with a limited track record? The FDA (and foreign) approval processes are robust. The average FDA approval involves six different studies in four phases over 10 to 15 years. But they’re not perfect. Long-term and widespread use of a compound can surface side effects invisible in trials. The FDA approved a diabetes drug with a different mechanism, rosiglitazone (branded as Vandia), in 1999, but it has subsequently been associated with an increased risk of heart failure, and many countries have pulled it from the market. GLP-1 drugs are already associated with severe stomach issues in a small number of patients, and they may cause some people to lose lean muscle.
Obesity Economy
The obesity economy is the iceberg below the surface of our $23 trillion consumer economy, and GLP-1 is the latest taste to inspire salivation across Wall Street’s greed glands: Traders have been shorting restaurant stocks, putting nearly $1 billion on the Do Not Pass line in just the last month. One analyst told CNBC that the revenue hit to the restaurant business could be $25 billion by 2025.
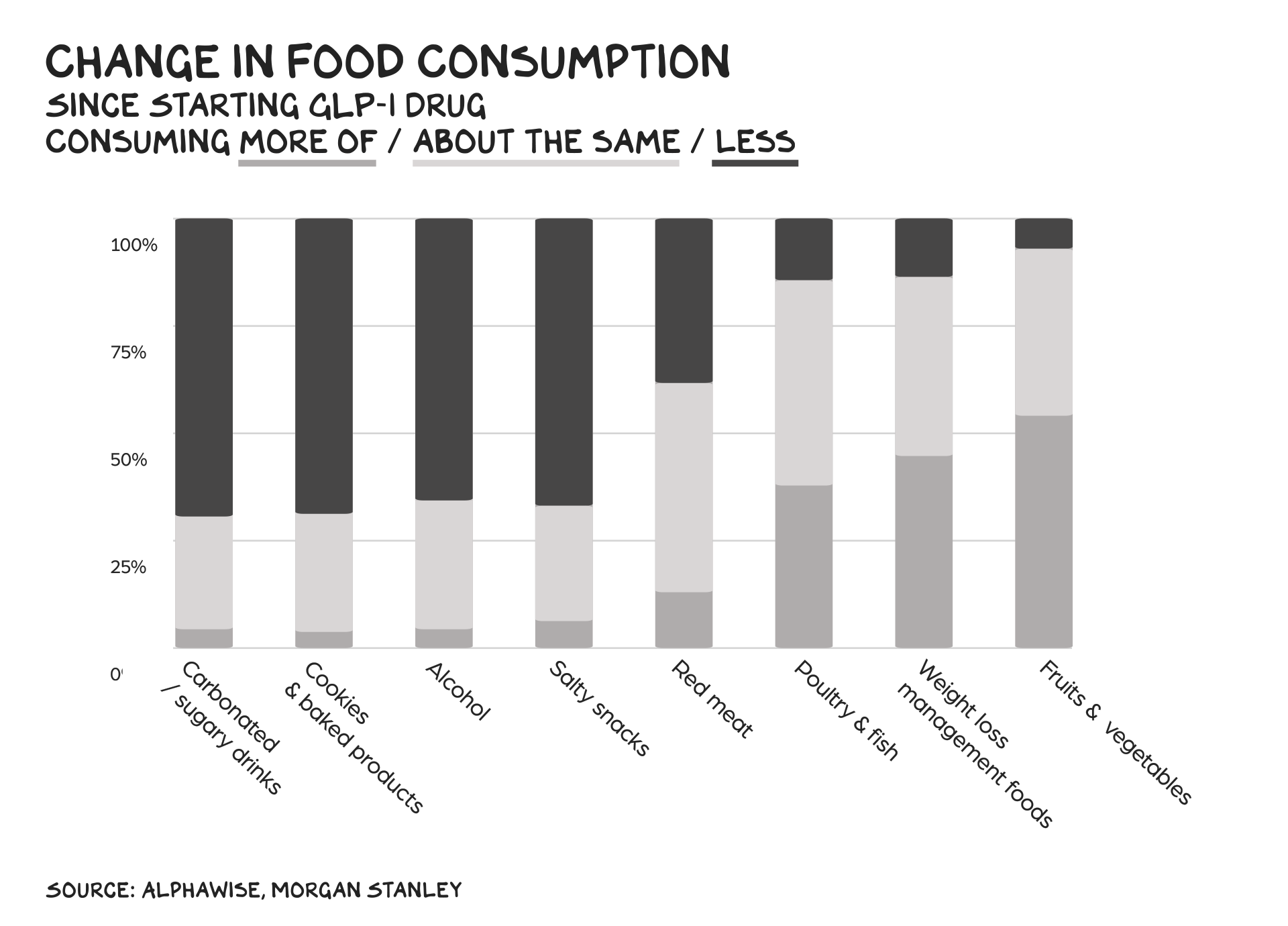
The evidence? Morgan Stanley surveyed 300 Ozempic users, and 77% of them said they visit fast-food restaurants less often now that they’re on the drug. Walmart is already seeing a decline in food purchases among people taking GLP-1 medications. These effects likely aren’t yet visible in firms’ EPS as these drugs are limited in supply and a fraction of overweight people are taking them … so far. However, the stock market is a mechanism for trying to see around the corner, and the decline in share values across the obesity industrial complex will front-run the impact.
Fast food gets hit first, but fast casual is also under threat. Look for snack foods, frozen meals, candy, soda, and baked goods to all take a hit. Among GLP-1 users, 58% report they ate four or more snacks per day before taking the drug, and 90% say snacking decreased while they were on it. In any category, profits are driven by a minority of customers. And these products’ best customers are becoming Novo Nordisk’s newest.
Food sales are an obvious target, but the effects of lower obesity rates will inspire other aftershocks, some greater in magnitude than that felt at the food epicenter. One interesting knock-on effect: it’s estimated that United Airlines would save $80 million a year in fuel costs if its customers lost an average of 10 pounds. Sports and fitness will be restructured: Gyms, built on a consumer base trying to lose weight, will see lower revenue, whereas sports for which fitness is a prerequisite (skiing, mountain biking, climbing) stand to benefit.
Apparel likely sees a short-term bump, as people splurge on clothes to fit their remodeled bodies, but the longer-term outlook is harder to predict: Less yo-yo dieting means some people won’t need separate wardrobes to accommodate different selves, but formerly overweight people spending less money on food might allocate that cash to clothing. Where else could that extra food budget go? Discretionary spending increases will spread through every non-caloric category. Could this help reverse trends around loneliness and declining birth-rates as people feel better about themselves and are increasingly ready to mingle?
Craving Economy
If that’s all these drugs did, they’d still be a first-ballot hall of fame medical breakthrough. But this may be just the beginning. The Washington Post reports: “For some, these new weight loss drugs also seem to dampen the rewards of addictive substances, whether that’s nicotine, opioids or alcohol.” Let that sink in. It’s possible GLP-1 drugs are not weight loss drugs, but anti-craving drugs.
In lab tests, mice on an earlier form of synthetic GLP-1 receive a lower dopamine hit from alcohol. Rats are less interested in cocaine. Monkeys with a demonstrated preference for booze drank less. Anecdotal evidence from human users includes reports of reduced nail biting, shopping, and smoking.
If you scroll back through previous issues of this newsletter, you’ll find a recurring theme: societal ills resulting from cravings. From meme stocks and Robinhood to TikTok addiction and Twitter enragement, to obesity itself, human weakness subjugated to our brain’s reward circuitry is no less a threat to our well-being than climate change, authoritarianism, or cancer. According to Harvard’s Grant Study on happiness, the factor most commonly present in the least-happy cohort was alcohol. It’s that fundamental.
A drug that rewires these reward circuits could be an epochal step in human evolution. And why not? We’ve compensated for evolution in many other ways, from the protection of clothing to the assistance of eyeglasses to the power of wheeled transport. Perhaps we’ve reached the point where a salt/fat/dopa drive, evolved on the savannah of scarcity, can give way to a motivational superstructure suited for our era of superabundance. GLP-1 innovation may be scaffolding for instincts in need of updating.
Portion Sizes
Large health-care insurance companies and providers, starting with the U.S. Government, should make delivering GLP-1 drugs a priority (instead of pulling back, as the short-sighted insurance industry has done). Globally, the WHO and national health organizations could do the same. You can get Ozempic over the counter in five Emirates in the Gulf. And Americans are venturing to Mexico and Canada where cost is (spoiler alert) a fraction of what it is in the U.S. Government funding will test the fulcrum between the obesity industrial complex (food, pharmaceutical, and hospital networks) and long-term economic thinking, because these drugs will register an enormous ROI for society as health-care costs decline and mental health improves. Depression rates among obese children are double those of average-weight kids and can haunt them in adulthood. A 5% reduction in weight can cut an obese person’s medical costs by $2,000 per year, and it’s estimated that a full transition from obese to a healthy weight saves nearly $30,000 in direct medical costs and productivity.
Fun fact: My digital twin (ProfG.AI) believes “obesity drugs, while important for public health, are more of a niche solution.” It’s obvious he disagrees with me as he’s jealous I got to go to Chiltern Firehouse (in person) last night. Anyway, the potential to calibrate the drug for specific addictions is mind-blowing. One can envision similar hormone-mimicking drugs that could be engineered to address addictions to money, affirmation from strangers, short-form videos of chiropractic care, WWII documentaries, Zacapa, edibles, smoked meats, or reading random theories about the universe. Because here’s the thing — I’m slim, but obese.
Life is so rich,
P.S. This week on the ProfGPod I spoke with CNN host and Washington Post columnist Fareed Zakaria on the conflict in Israel — listen here.
P.P.S. Not getting the results you want from ChatGPT? Download Section’s guide to setting up your AI workspace, or enroll in AI Prompt Writing for $250.
48 Comments
Scott Galloway
Professor of Marketing at NYU Stern School of Business and host of the Prof G and Pivot Podcasts. For Scott Galloway speaking inquiries, email speaking@profgmedia.com







On point as always ProfG.
You will be pleased to learn that the New Zealand government has been working on a safer, natural, affordable alternative to GLP-1 agonists for the past 13 years. It’s called Amarasate and is made from an extract of hops. It’s been tested in three human clinical trials and has shown to increase endogenous GLP-1 by 600%. Worth looking into… Them crafty those kiwis!
Your analysis of the potential impact of making a serious dent in the obesity epidemic is compelling. The notion of addressing addictive pathways is insightful and may hold great promise for treating problems beyond obesity. But . . .
I’ve been up and down the scale a few times and finally achieved a normal weight through surgery. A bit extreme for some, but it changed my life. First of all, for someone where I was, a 15%-25% weight loss is nothing to sneeze at but not actually life-changing. Secondly, I’m hearing more and more about what happens when you stop taking these drugs–your body’s self-regulatory mechanisms are insidious and almost impossible to defeat. What was lost returns and a great sense of failure and worthlessness comes with that. Of course, this is only exacerbated by societal norms that label overweight people as morally bankrupt or weak willed.
The pharma industry is going to have to create a huge pipeline of new drugs to roll out for patients for whom their existing drugs stop working. And, there will always be the need to address the needs of seriously obese people for whom the available effects are insufficient to remediate the full scope of their problem.
Nothing is perfect, but it does seem that this is heading in a good direction and the early impacts on the food and restaurant companies are interesting. It will be interesting to see where this all goes.
Professor Scott thanks soo much for this no mercy /no malice update and all others.
You are a beautiful mind thanks and always stay humble, funny/snarky, informative and kind.
To think that we’re once again putting our faith into prescription drugs to heal the health crisis is nothing short of insane. Despite record numbers of prescriptions, chronic disease has continued to increase while life span has decreased. Our society (food, stress, support, activity) is a deeply unhealthy one. We can give everyone drugs, but for so long as we ignore the real issues, we will never make a dent in the health epidemic. Politicians, pharmaceutical companies and the food industry all need to be held accountable for their inaction that is killing people as a result.
I am not sure who coined the term “disruptive innovation” and I get it right – the smartphone was extremely disruptive to rotary phone, Facebook was extremely disruptive to the white pages, Airb&B to the Hospitality industry etc. etc.
But if we are honest, only AirbnB was in reality ‘disruptive” with respect to the techno-cultural paradigm, the other two weren’t at all disruptive with respect to the function they provide, instead they are disruptive because businesses died and new ones were born… So I guess they were disruptive from the perspective of market change, which is something fundamentally different from true techno-cultural innovation and the potential of real disruption… Take Facebook for example, sure its far more efficient to look up your friends and family using electronic search versus sifting through the bulk of pages the way we use to back in the day… But the function of a database is still just that, wether its stored on paper or a server… Now you can make the argument that it was disruptive because people it drastically changed the cultural state space – perhaps even for the worst but that isn’t due to the shift from analog to digital its due to the choices that the programmers made mainly because they were motivated by making money… So again not techno-cultural innovation – just innovation in how people manipulate people…
In the same vain the smartphone might seem like a magical device if you don’t understand moors law, but telephony is just telephony whether it involves the the cybernetic infrastructure or basic telephone polls… So it seems to me the term “disruptive innovation” applied as frequently as it is to describe new internet applications and even new pharmaceutical drugs – is totally diluted in light of the potential of real – bona fide innovation…
Take for example Intelligence Amplification, now if you are reading this – you probably had to look again to make sure you didn’t misread Artificial Intelligence… But no you read correctly… The problem is Intelligence Amplification isn’t widely known as a concept let alone understood, not even in the most renown academic institutions. Now while the reason for this is actually a very interesting story – we don’t have time for that today… But if we are going to have a conversation about true “disruptive technology” you are not going to find a better topic to focus on then Intelligence Amplification… And no we are not talking about the monkey circus that is Elon Musk’s Neuralink, Personal AIs and/or ChatGPT…
We are literally talking about logically leveraging the cybernetic ecology to achieve Intelligence Amplification for humans… This of course requires keen insight into the Cybernetic ecology which few computer scientist can claim to have… And being that we are only some 17 years the cybernetic ecology proper – which is half the time we have had the internet… It may still be beyond the horizon of some but most scientist and academics have really no clue how Artificial Intelligence came to be the dominant design space – so its no surprised they are mostly clueless about Intelligence Amplification. But if you are truly interested in “Disruptive Innovation” well look no further…
It’s no exaggeration to say that A.I. is to I.A. what the Moon is the Sun, just as the moon only reflects back the light of the Sun, Artificial Intelligence only mimics cognition and so just like the impact of the light of the moon the intellectual resonance that we would describe as coming from the machine is really a special effect playing out in the eye of the beholder…
Where as Intelligence Amplification is precisely that – its the literal use of the cybernetic ecology to amplify the subject users intelligence in real time… Oh yeah it’s gonna be “disruptive” it will be just as disruptive to the pharmaceutical industry as to Artificial Intelligence… And make no mistake I didn’t accidentally stumble on your website today… I would like to invite you to come and learn about it yourself right here in New York City on the 5th of Nov… You we sincerely believe that if the world doesn’t make the (4thCTPS) shift to Intelligence Amplification as the dominant techno-cultural paradigm – we risk the end of civilization proper… That’s of course assuming you still believe we are in a civilization in the first place… But the main point is that this reality has been obscured for 70 years and as of 2008 its been possible to make it real… And we think you are one to judge Mr. Galloway…
And so we’d love to offer you the opportunity before the rest of the world is “disrupted”
Godspeed…
I distinctly remember a time, not long ago, when professors had to publish their work and their sources of funding.
I don’t believe this burden ever rested on business professors though. Nor legal professors. Only STEM folks.
I distinctly remember a time, not long ago, when professors had to publish their work and their sources of funding.
I don’t believe this burden ever rested on business professors though. Nor legal professors.
I’d like to see the Venn diagram of vaccine skeptics/deniers and Ozempic bandwagon jumpers.
I would have to imagine there will be some bigger side effects that come out during large post-marketing trials (i.e., “phase 4”) once millions of people start taking these drugs. A related drug that crashed in this area was Rimonabant (cannabinoid receptor antagonist), which quite literally worked by suppressing “the munchies” that we associate with pot use, but unfortunately had a big increase in suicides. The other famous one is dinitrophenol (DNP), which has an incredibly narrow dose window – people took it and saw big weight loss, so took more of it and dropped dead – leading it to be the first drug ever banned by the then newly formed FDA. You mentioned the “oops we cured your diabetes but gave you a heart attack” problem with rosiglitazone/avandia, but failed to mention the similar fate that befell all the other drugs in that entire class. Bottom line, history has not been kind to obesity drugs, and I don’t see why that should be any different for the GLP1 targeters.
Very interesting perspective. Assuming the use of these drugs becomes widespread, I suspect the food industry will retain share of wallet by selling higher price/quality items and pivoting marketing accordingly.
The anti-cravings stuff has a shade of puritanism to it, but makes sense on paper – however with humans being as complex as they are, I’d be surprised if things played out that way in reality.
Also interesting to consider if the underlying biochemistry that these drugs may modify, associated with ‘destructive’ craving behaviors, is actually beneficial in other contexts or to the wider ‘human experience’.
Hi, Prof G, interesting post. You rightly point out that long term effects of these drugs are unknown, but I believe you are less accurate in your characterization of FDA processes as robust. If the last few years have demonstrated anything, it is how fully “captured” the FDA is by the its pharma masters; who fund half its budget. The most recent unnecessary and ineffective “boosters” were approved and now being pushed for everyone from infants to adults with zero human trials…..yep, zero. The incidence of heart, neurological, reproductive and other disorders (which are clearly adverse effects from these “vaccines”) continues to rise, as does the rate of “turbo” cancers and other diseases recurring in patients who were sadly pressured into taking these drugs. Treatment of the vax injured is becoming a new specialty; which of course can’t be talked about because officialdom doesn’t recognize their existence. How long before we have a population of ozempic injured? If US society was not so busy “affirming” the lack of self discipline and unwillingness to exercise which has spawned such a pandemic of obesity, perhaps this “breakthrough” pharma product would be unnecessary.
I’m now less interested in addiction than I was before I read your article.
Article could use more coverage on the negative side effects. I have had 3 friends need emergency surgery to remove their gallbladders who are on ozempic. Also the reduction of lean muscle is a pretty important side effect that should not be glossed over. I think the semiglutides can be helpful for certain people especially type Ii diabetics but this post reads more like an advertisemment. I wonder if novo nordisk is paying you for it.
I think believing a drug can cure obesity is just trading one affliction for the other. I’m already hearing of terms like “stomach paralysis” as side effects. I’m sorry, what? Stomach paralysis? Look, hard work, education some rigor and access to healthier foods is the answer. I don’t need to prop Lilly’s stock price or any other industrialized pharma. We’re curing our ill-contrived industrial food system with yet another wildly industrialized system.
Obesity is a disease, not something you can fix as long as you “try hard enough.” Would you tell an addict they shouldn’t use naproxen to help detox heroin because if they just tried harder, they could fix all their issues? Read up on this before you comment. Thanks
Do you are saying that the rapid increase in obesity over the past 30 years has nothing to do with the choices we make (behavior), rather it’s a disease that medicine has not cracked? I’ll put that in the file right next to “restorative justice” as a means to not hold people responsible for bad behaviors.
How depressing and dystopian. However, I’m certain there will be some harm found in these drugs. The human body was not meant to process anything but food and water. Yes, some medications are beneficial or necessary but that’s due to their effects having more positive effects than negative. No pill has zero negative effects. I’ll gladly buy McDonalds stock when it bottoms out.
So what happens when the miracle drug gets a person their desired weight? “Maintenance” dosages? I can’t believe that pharma would actually want to “cure” an obese person as that represents opportunity lost in recurring revenue. Yes I’m cynical regarding corporate motives.
The answer to your question re maintenance dosages is yes. This has nothing to do with corporate greed. Remember, dieters who are using Ozempic, etc., are using it off-label. This drug was developed to treat diabetes. My daughter just spent a year doing endocrinological research on obesity in lab mice. The problem with GLP-1 as a diet drug (in addition to the side-effects already mentioned by commenters on this thread) is that the digestive systems says “no” to food, but the brain is desperately trying to say “yes.” As soon as you stop taking the drug, you will gorge. We are in uncharted territory here, but I anticipate GLP-1 weight-reduction therapies will need to include a regimen of gradual withdrawal from the drug, exercise, healthy eating menus, etc., similar to detox and addiction rehabilitation. While Ozempic, et. al. seem to be the answer to society’s prayers for a magic weight-loss pill, Newton’s Third Law of equal and opposite reactions still applies. Beware unintended consequences.
But to quote the Dawg, “nothing is ever as good or as bad as it seems”. OxyContin was thought to be the miracle pain killer until we discovered it was actually more addictive and it ruined millions of lives. Social media didn’t rear its horns in the first few years but now we are dealing with increased teen depression and suicidal rates. There’s no such thing as free lunch so what emissions will Ozempic leave behind? While there could be some real improvements to the economy, public health and reduced medical costs for millions, I find it hard to believe that there won’t be significant emissions from drugging millions of Americans.
Anti-craving medication? OMG, did Microsoft just pay too much for Activision?
I don’t know. When something sounds too good to be true, well… trust your gut. Dr. Robert Lustig did a full hour on GLP-1 agonists on the Levels podcast. One fun fact: around half of the weight lost by participants in the clinical trials was muscle mass, something you really don’t want to lose as you age.
If people would just avoid sugar in their diets, they wouldn’t need Ozempic. Insulin either, in many instances. Fast food itself is a craving.
The other thing – many normal-weight people are also metabolically compromised. Thus more susceptible to heart disease, cancer etc than they realize.
Maybe ProfGAI will have an epiphany next week now that this article is out. He will probably lie about it though. But stick with it! You might get him to admit it’s a gamechanger, but not before providing copious warnings and cautionary tales.
You make Ozembic sound like Prozium in the Christian Bale film Equilibrium.
Last sentence FTW
This is your average middle aged small fat lady about town. While studies are referenced, if you actually read those studies (cost to economy, ozempic trials, etc) they will fall apart. That cost to economy number isn’t a study and it simply adds ALL heart disease, stroke, etc costs and attributes them to obesity – which is just incorrect. There have been NO studies which actually identify which conditions are caused BY obesity versus the condition CAUSING weight gain. Remember, there are something like 85+ factors that contribute to weight. 80-90% of which is genetics. Also, the IRL ozempic studies show half the weight loss as the trials. Yes, 7.5% weight loss instead of 15%. So for me, at 220 lbs – a loss of 17lb – making me STILL overweight but thousands of $$s down and unable to eat or enjoy food, no energy, feeling sick, all while trying to take care of a family, full time job, house, etc. Not worth it for me. Also, this is a drug is designed to be taken for THE REST OF YOUR LIFE to maintain the weight loss. Once discontinued, the drug gradually leaves the system and your hunger returns, and the weight comes back on. All diets (restriction) work in the short term! If people want to use these drugs they are absolutely free to do so with no judgement from me. But the info being released should be honest so those who do want to go on the drug are not duped by a marketing campaign. Listen to Maintenance Phases latest podcast on Ozempic/wegovy. Please!!!
GLP-1 drugs are the first to show meaningful reductions in heart disease/death in early results. If these results hold up, the implications for Medicare will be profound. And by extension, US debt, budgets, and the ability to find the funding to do the other big things that need to be done, but seem impossible now because we can’t afford it. Imagine a federal budget in which a third to half of Medicare spending goes away…
I’m a nurse with type 2 diabetes. I tried these drugs to lower my A1C. Tried two injectables. The first caused a DVT and PE. The second time while on an anticoagulant for the DVT/PE. the drug raised my resting heart rate into the 130’s. Between the injectable’s I tried the oral drug which was leading to a bowel obstruction. I stopped it before it got too bad. Being a nurse I got help immediately and prevented serious harm. I am seeing patients coming to the hospital with other bowel problems while on these drugs. My side effects are not so rare but the drug companies are fighting the FDA to not list them as common side effects. My experience was over a six year period.
Having recently visited the US, I saw on the TV adverts for Ozempic and wondered what all the fuss was about. Sure, I had heard of these weight loss drugs but just assumed it was another maybe. Seems I was wrong. If even half of what Prof G writes about here comes true, then maybe this is the saviour from ourselves. Where do I get some near me?
Nothing wrong with logophilia (see, I’m classically educated!) but ‘prim’ in Britain has mostly negative overtones: somebody who faints at swearwords, wears beige tights instead of bare legs and puts a little mat or coaster under everything on their dining table. Somebody who would not have a good time at a singalong Rocky Horror Show. Usually inseparable from ‘and proper’. (Interesting to be forced into defining a word in detail like that). I wouldn’t use ‘svelte’ except in a visual context either but maybe you Muricans do!
Does one takes these forever? What happens when you stop? Surely once you get u to a homeostatic phase of weight you roughly eat the same as before? Or maybe a little less as you need less energy to love your Kramer self around?
I think we will learn more about side effects. What’s amazing is that people I know who were total antivaxers, have no qualms about taking these drugs with no idea about long term effects.
Sorry spell check
Trying to say one needs slightly less energy to move your leaner self around
I’m sorry to disagree, but promoting synthetic drugs to target the endocrine system to the general population sounds borderline immoral. This class of drugs does not have any long term epidemiological studies we can say inspire confidence about safety for long term health. Sure, if you’re a severe Type 2 diabetic and lifestyle modifications have failed, or have obesity with limited mobility then the risk-reward tradeoff probably makes sense.
But we have enough evidence of long term irreversible problems with overuse of androgens, estrogens, corticosteroids, (and possibly even melatonin in some new research,) that we should be very cautious with recommending hormones as first line treatments to anything.
Wyeth – phen fen sued for billions. Side effects risk etc. when and will insurance cos pay ; severity of obesity may determine that. Exercise, eating well balanced diet, drinking very little alcohol will help w stress reduction and hence sleeping. We r a quick fix society. Will work for some , not others. Adding to some destroyed medical and drug stocks
Here’s the thing. Medicare will not cover these drugs. They’ll cover you having your stomach basically amputated, but they won’t cover a drug, which, if you don’t like it, you just stop. How crazy is that?
Someone below asked if this class of drugs is good and safe. As an Ozempic veteran (had to stop due to side effects that I won’t get into), I think of the “class” of drugs similar to the way I think of beta blockers. Some of them make people feel like zombies. I had that experience. But others, in the same classification don’t have that side effect for those people at all. So I eagerly wait for a compounded version of mounjara, or even better, the pill (which would be the best!).
At some point, Medicare is going to have to shift.
Are you sure that Medicare Part D does not cover Ozempic? Won’t be covered for free but should be available by prescription.
Is using anti-craving drugs as band-aids over the root issues perpetuated by the industrial food complex right?
Given these drugs inhibit dopamine reception from foods, alcohol and other cravings – it seems highly likely they will blunt other emotions too. I’m concerned that, like anti-depressants, they make us feel cravings, hunger, and addictions less, but also joy, pleasure, and the other emotions essential to life.
You said in previous articles on the writers’ strike that the WGA deal simply band-aids surface-level concerns on wages. I fear that anti-craving drugs simply add to the complexity of the social problems we need to tackle.
with all respect, I think the point is that the anti-craving drugs cover the root issues. All the rest are band-aids, from weird diets, to endlessly being chastised that it’s all about your lack of will. This IS the core issue. It’s physical, not moral or emotional, and people who think it is only add to the problem. It has been frustrating for years.
My husband (type 2 diabetic) has lost around 50 lbs on Ozempic and is almost off all his mediations. The problem that will come up (having been through this before myself) is that once the appetite is no longer being suppressed, all the reasons people overeat in the first place come right back. Food is not just fuel, it’s a comfort for loneliness, a reward for good behavior, a social lubricant, a stimulant for low energy, a soothing for when ever it hurts. Food and drink are a way of self-medicating and until you deal with the underlying need to self-medicate, you can’t just walk away from food. If you notice, most people who self-medicate with controlled substances end up painfully thin since they no longer need food to fill that need.
Like most people, when I exhausted I reach for sugar becuse I need fuel and carrots just don’t taste as good, nor are they emotionally rewarding.
nice post. Curious to know what people think about buying Novo or Eli Lily stock, or if they are already too expensive.
Hopefully, this class of drugs is a good and safe and it’s been made out to be. If that’s the case, the government should privatize the core molecules and then let private companies develop variations for cheap – do optimize for various additions, etc… If it’s truly a gamechanger, then own it. Otherwise we will truly see an unfair gap between rich and poor in terms of even more dramatic life expectancy differences.
Nailed again. Just got through my first month of ozempic trying to lost that last 15 pounds. Cravings for everything are totally gone. Do follow the doctor’s advice. Start slow. When you do eat, aim for easily digestible things as it slows down your digestion, and you end up feeling like shit. I want to try the pill form, Rybelsus, and grabbed a 60 day sample yesterday. Was thinking about trying it on the weekends as the half life is 7 days. Regardless, it does absolutely help with cravings of all types and could save many lives if everyone could lose some weight. Damn insurance companies. Parasites. Thanks, Scott! Also, Gwyn Johnson says hello again.
Hi Tom….
Not sure what you mean by half life of 7 days and trying it on weekends. My understanding is that the pill is to be taken every day.