


America’s Best Bet
America’s Best Bet

Audio Recording by George Hahn
America is now one giant bet on AI. If not for the Magnificent 10, the markets would be flat for the year. There’s a different technology that offers more asymmetric upside. If we want to transform the economy — and the well-being of Americans — we should focus on GLP-1, not GPT-5.
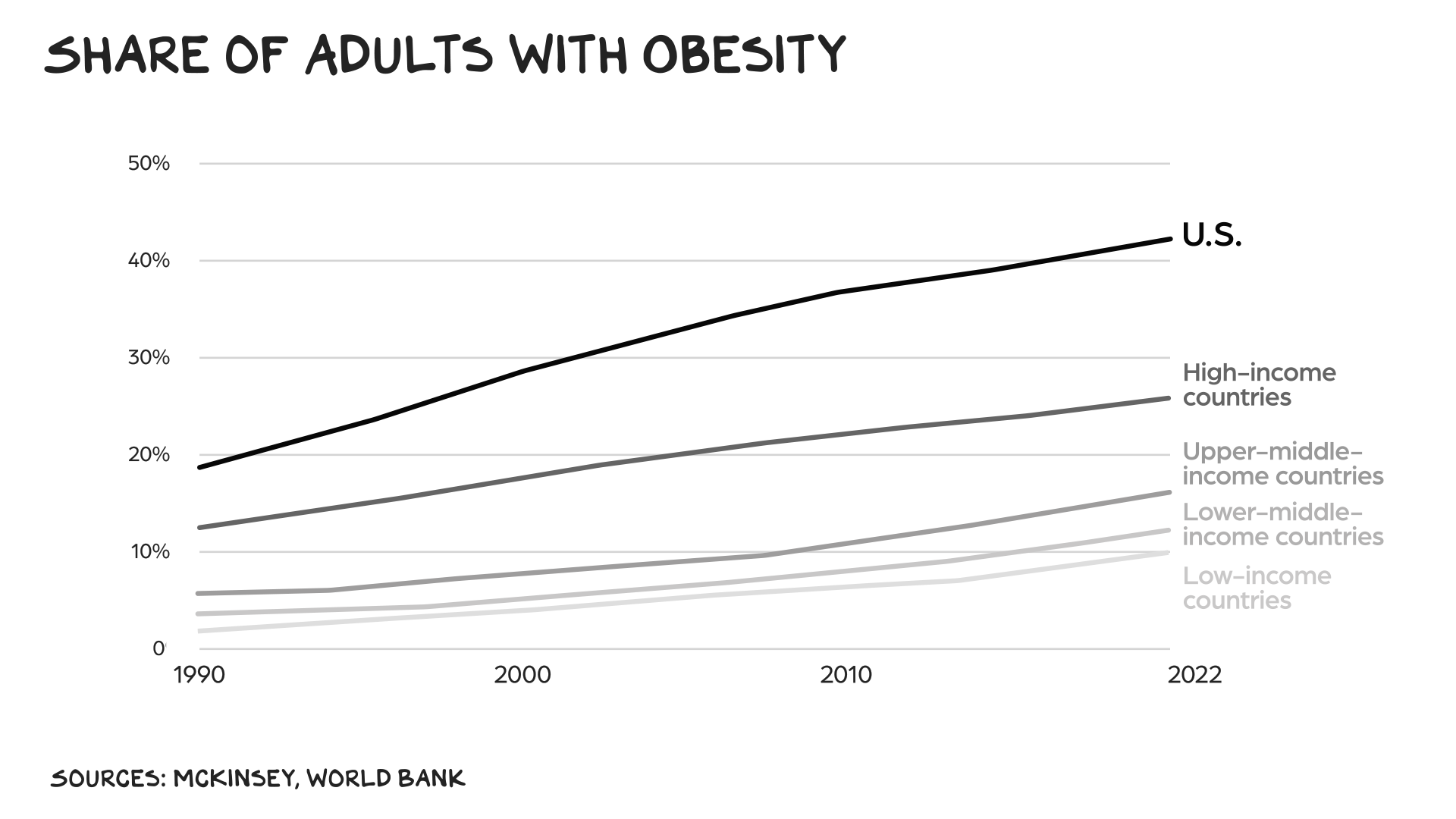
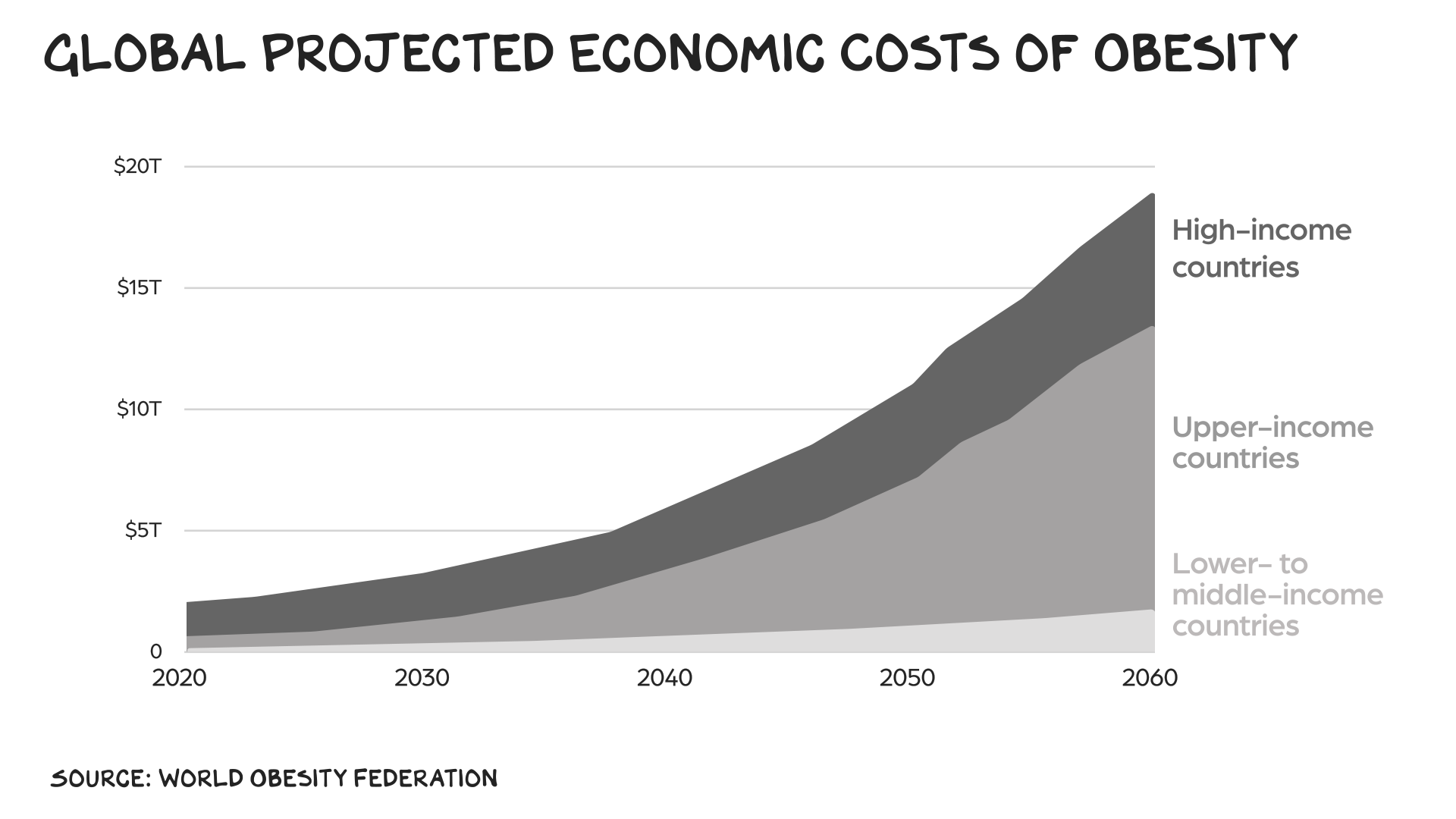
More than 40% of American adults — 100 million people — are struggling with obesity. By 2060 half of U.S. adults may be obese. The healthcare costs of all that extra weight could exceed $20 trillion over that period.
Our debt — $5 trillion in receipts vs. $7 trillion in spending — has become the IED of our economy. We don’t know when or why it will detonate. If we’re going to have an adult conversation re spending, all roads lead to the same place: healthcare. We spend $13,000 per person, versus $6,500 in the rest of the G7. Matching the efficiency of our peers would save us $2 trillion a year.
Why do we spend double to die sooner, while experiencing more anxiety, depression, and chronic illness? Our problem isn’t vaccines, food dyes, or Tylenol. It’s fat. The Milken Institute and McKinsey have estimated that obesity costs us about $400 billion annually in direct medical costs and lost productivity.
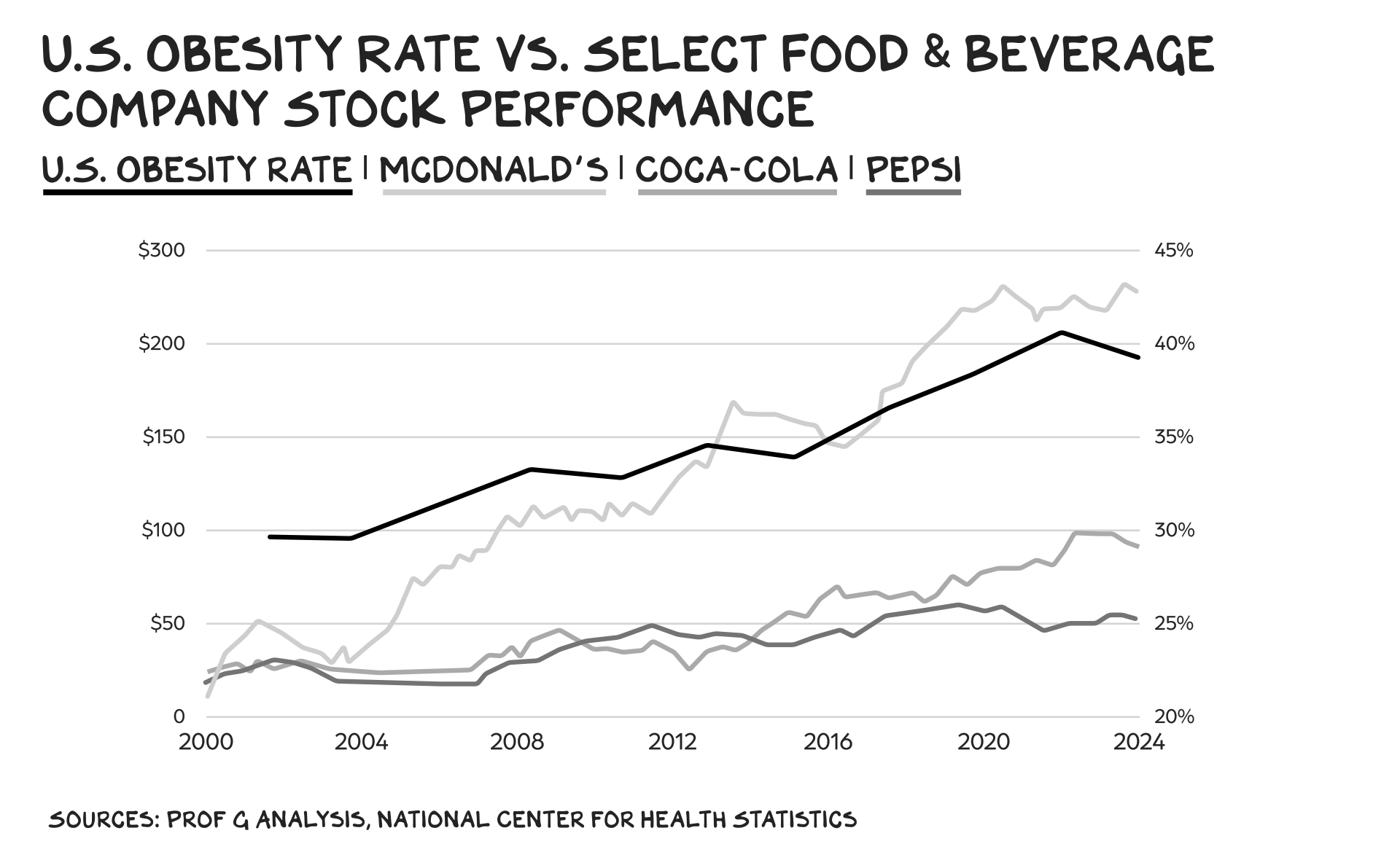
U.S. healthcare isn’t about caring for health — it’s about monetizing it. Just as Big Tech found the gangster app for shareholder value (rage), the industrial food, hospital, and pharma complexes have found obesity. They get you addicted to sugar and salt, then hand you to the “non-health” complex for replacements, dialysis, and statins. They’ve even rebranded disease as identity: You’re not obese, you’re living your truth. No — you’re finding diabetes. McDonald’s and Coca-Cola celebrate obesity so UnitedHealthcare can monetize it. These stocks aren’t equities; they’re obesity indices.
We know exercise, healthier food, and less screen time help. But they’re not enough. The good news: Obesity may have peaked in the U.S., and we have the tools to actually reverse it. Pushing for a radically lower price and rolling out weight-loss drugs to tens of millions of Americans could be revolutionary — possibly the best civic investment in recent history.
Sticker Shock
In sum, our instincts have not kept pace with industrial production, and we gorge. GLP-1s put scaffolding on our instincts. Most of us have friends or colleagues we barely recognize after they’ve taken novel weight-loss drugs. By mimicking a hormone called GLP-1, the medicines suppress hunger and make us feel fuller longer. The results are dramatic — 15% to 20% reductions in body weight — yet uptake remains small relative to the tens of millions who could benefit.
Coverage is patchy. Only 30% to 40% of commercial plans and 14 state Medicaid programs cover the cost of GLP-1s for obesity. The administration is considering a pilot to expand coverage under Medicaid and Medicare — a shift in policy after rejecting a Biden-era plan that would have cost $35 billion over 10 years.
Prices need to fall for the math to work. If Medicare began covering GLP-1s, researchers estimate 3 million beneficiaries would start using them over the next decade at a gross cost of $66 billion and savings (in avoided healthcare spending) of $18 billion — for a net price tag of $48 billion.
Price Cuts
Costs are moving in the right direction. Wegovy and Ozempic now run under $7,000 a year; Costco offers a monthly supply of obesity drugs for $499; and competition from Lilly and others is driving prices down. More than 100 next-generation obesity drugs are in development, including pill versions.
President Trump on Oct. 16 vowed to slash GLP-1 prices to $150 a month to match the expense in other developed nations, but no deal yet exists with drugmakers. Investors, however, took him seriously: Shares of Novo Nordisk and Lilly dropped sharply on the news.
Economist Emily Oster argues the budgetary worries of expanding access are overstated. Medicaid tends to pay far less than private insurers, and a “typical” 53% discount could drop monthly costs to $235. If 10% of eligible patients took the drugs, it would raise Medicaid spending by just 0.4%.
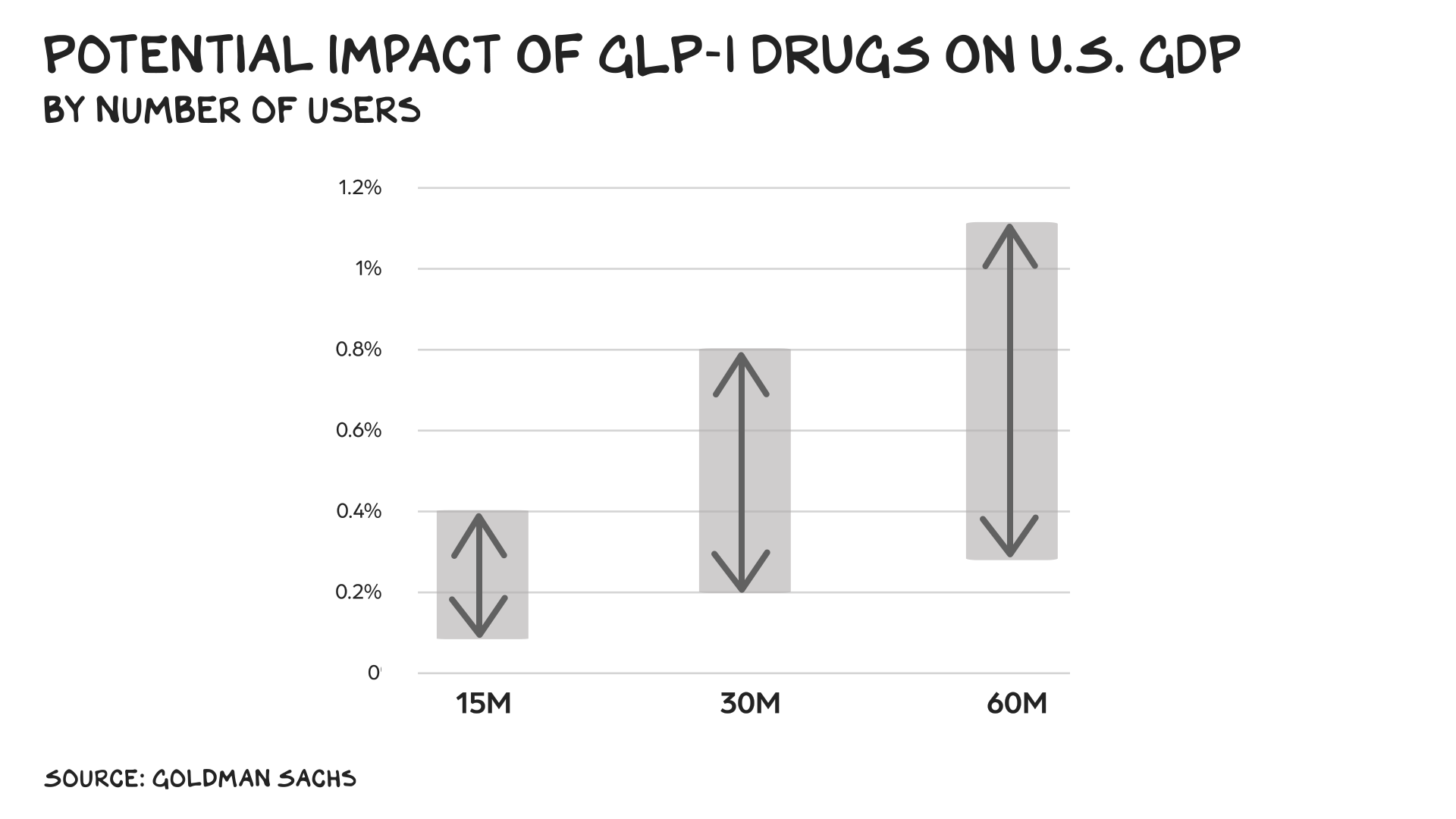
The concerns also miss the upside: About 5 million U.S. adults use GLP-1s today. If 30 million did, Goldman Sachs estimates GDP would rise as much as 0.8%. At 60 million, the increase could exceed 1%.
Global Weight Class
America isn’t the only country fighting this epidemic. In Britain, obesity costs the economy £31 billion a year in lower productivity, sick days, and early deaths. “We’ve created a food system that’s poisoning our population and bankrupting the state,” says Henry Dimbleby, co-founder of Leon restaurants, which bills itself as a purveyor of fast but healthy meals.
Defusing the Food Bombs
These drugs aren’t a silver bullet, but they are a bullet. Many people quit taking them within a year or two, often because of cost or gastrointestinal side effects, and lasting success still requires exercise and diet changes. But alongside those measures, GLP-1s may be the key to fighting a complex disease rooted in physiology, environment, and policy as much as behavior.
In a society addicted to ultra-processed food and sedentary hours lost in front of screens, we need new weapons. Former FDA commissioner David Kessler calls GLP-1s a way to “defuse the ultra-formulated food bombs” that have hijacked our health.
RFK Jr. has called for “lifestyle” changes while cutting NIH funding — the moral equivalent of telling people to lift weights while closing the gym. The administration’s “Secretary of War,” Pete Hegseth, has shamed “fat generals” but offers no help other than performative masculinity.
Bending the Curve
Scaling access could prevent adult obesity from topping 50% — and push it back toward 30%. Giving 10 million Americans GLP-1s and lowering their monthly cost to $50 would run $12 billion over two years. That’s a bargain. Targeting the patients most likely to benefit would improve returns further. Obesity shortens life expectancy by up to 10 years, partly because it increases the risk for more than a dozen types of cancer. Reducing its prevalence would yield massive health and productivity gains over the next 30 years. I’m sticking with the thesis I shared with Bill Maher two years ago: GLP-1s will have a bigger impact on the real economy than AI.
The Cost of Inaction
OpenAI’s Sam Altman calls Sora “the most powerful imagination engine ever built.” In reality it’s an endless feed of digital slop, further blurring the truth. The real engine of progress comes in a syringe. Maybe we should put it in the water.
Researchers are aiming to preserve muscle and overcome one of the drawbacks with the first treatments, or eliminate injections altogether. They’re also testing GLP-1s to treat conditions beyond obesity. Novo Nordisk is betting its drugs can work against Alzheimer’s. Whether or not these efforts succeed, the trajectory is clear: This technology could reverse the most expensive disease in history.
America’s two great growth engines are rage and carbs — AI monetizes the former, the food complex the latter. GLP-1s may finally break the loop: shrinking our waistlines, cutting costs, and reminding us that progress isn’t digital, it’s biological. The next great platform isn’t the neural net — it’s the needle.
Life is so rich,
P.S. On Raging Moderates this week, my co-host Jessica Tarlov spoke with David Frum of the Atlantic about the Democratic Party’s predicament — and the value of tacking to the center.
Listen here on Apple or Spotify, or watch it here on YouTube.
47 Comments
Scott Galloway
Professor of Marketing at NYU Stern School of Business and host of the Prof G and Pivot Podcasts. For Scott Galloway speaking inquiries, email speaking@profgmedia.com







Google is by and by paying $25375 to $28548 consistently for taking a shot at the web from home. I have joined this action 2 months back and I have earned $31547 in my first month from this action. I can say my life is improved completely! Take a gander at it what I do.This is what I do………………………….www.tagsalary.agency
The basic premise, that Americans need to eat less and reduce obesity, is supported in the literature. But there are some issues with this article. First, showing the obesity rate vs stock prices of the select food and beverage industry over time is the definition of bad correlational statistics. It’s the classic “more kids drown in swimming pools on days with higher ice cream sales” example. Your third variable is “time.” Had you shown the obesity rate next to the NASDAQ, it would have looked much worse, and I don’t think the NASDAQ is conspiring against people’s food habits.
Secondly, you ended the article by saying, “America’s two great growth engines are rage and carbs.” What? Over the past 20 years, carb-rich food sales have actually declined while low-carb, keto-friendly food sales have skyrocketed. Carbs are not the problem. Looking at food as macroingredients rather than food vs not-food (a carrot vs a 20-ingredient “keto bar”), is our problem.
In health the best medicine is always preventive. Meaning being proactive vs reactive. Why not focusing on solving the root cause? Scott, I would love to see the same approach as when you talk about AI companion products when you talk about Pepsi, Coca Cola and McD, where you question if we need those products, if there’s a net positive social impact beyond economic results. Why is not ultra processed food regulated?
What’s the positive impact of companies like Pepsi, Coca Cola and MCD? (An impact beyond employment and sourcing that could be easily replaced.)
Improved physical and mental health is vital for America in ways that aren’t plastered over by pharma. Last week, The Economist ran a story about a British grassroots initiative that’s spread around the world called parkrun. It’s a free 5K run every Saturday morning organised in thousands of parks and trails around the world by millions of people. The speed you complete it – under 15 minutes or over 50- is immaterial. parkrun’s trick is its consistency, regularity and social aspect. Volunteering and running milestones are formally recognised and people meet for coffee afterwards. Many peoples mental and physical health have improved immeasurably because of it. The US has proven largely resistant, (spending $50 on a ‘charity’ 5K with a medal and free bagel seems more appealing) but one has started at Brooklyn Bridge Park, so anyone in NYC can check it out next week, and for those policymakers in the beltway, there are several happening tomorrow. There’s more locations on parkrun.us (sorry to UK/IRE/GER/NED/AU/NZ/SA/CA/JA etc readers who are probably wise to it).
Scott, thanks for your insightful–and “on the mark”–comments and analysis. It is clear that the cost of these drugs could be brought down immediately (think the CVS/Novo deal as an example), and the benefits would be huge. Physicians and organizations have been promoting diet, exercise and plant based diets for years–but the public is enamored with other stuff, and many don’t engage in sufficient exercise to make a difference. Meanwhile, we watch obesity rates increase over those same years. We need a solution, and your probing comments offer the best rationale I have yet to see–aside from the research reports which continue to confirm the benefits of GLP-1 drugs. Keep up the great analyses and fearless commentaries!
Len, if you read my post and how parkrun’s been a successful public health intervention, check out one in your area. Atlanta’s well documented income/social/health inequalities would be aided by parkruns set up in deprived areas of the city.
Totally agree on the benefits of weight loss drugs and the power of a meaningful start (e.g. rapid and significant weight loss) to help people begin a lasting journey toward better health.
That said, the focus on buzz words like “ultra processed foods” over-complicates what is really a very simple fact. Americans simply eat and drink too much….of everything. Over the past 50years, the change in caloric burn has changed far less than the change in caloric intake. Working at a computer is not all that different from standing on an assembly line, and the more active trades (e.g. construction) are pretty much the same as they were then. But we have super-sized soft drinks, endless buffets, etc., and we snack all the time.
It’s easy to say “just eat less” The three easiest behavioral changes are:
1. Use a smaller plate at mealtime so the meal looks complete without having to pile it high and wide.
2. Slow down so that your stomach has time to tell you it is not hungry anymore.
3. Don’t snack.
Having read many of the comments it is clear that those who do not suffer from metabolic issues, do not have a clue what they are talking about. I’m 73. I’ve been on semiglutide for a little over 4 years. I was an early adopter having lost and regained over 250# in my adult life. My MD agreed and it has been a life changing experience. I’ve lost 25% of my weight and back to mine at 30. The food noise is completely gone. I don’t get hungry. I stop eating and actually feel full for the first time in my adult live. I can’t stand the thought of wine. If I eat something sweet it’s a tiny amount. The first 2 yrs were covered by Medicare but then stopped. Before I could find another source I gained back 20# in 3 weeks, the first 7 days, without changing my eating, I gained a pound a day. This says to me it impacts how my body metabolizes as well. I have felt “normal” for the first time in 50 yrs. I will take this for the rest of my life. BUT it is expensive and I am fortunate that while, not rich by any means, I can afford it on the compounding pharmacy market. My hope is that the price will come down as it’s recognized to dramatically help health in many ways. It is not for everyone, and ever body is unique. That said it has been a god send for me and I wish anyone that needs it can get it affordably. But you do need to take it for the rest of your life. If you quit your body goes back to what it was.
Suppose you own a factory that demands dependable manpower. Your employees need to eat so you add a cafeteria where you sell inexpensive, scientifically appealing (addictive) food at a profit. This food will also erode mental and physical health making workers less dependable and the factory less productive and profitable. You add an ineffective and unwieldy health care system that somehow still profits without resolving the problem.
Aha, you discover a medicine to remediate the effects of the addictive food AND you can sell it at a profit! Alas, many can’t afford it. Wait, what if you add a “sin” tax to the crippling food and use it to discount the medicine? Congratulations, you are an exemplary human! This is the greed based economy.
I agree with a lot of this article but if you do the research you may find that the GLP one miracle comes with massive and sometimes dangerous side effects. People who go on that for more than a few months they lose muscle and fat at a similar rate and also bone. It’s not a healthy way to lose weight. It’s definitely not recommended to just push out to millions and millions of Americans.
Certainly, it’s better than being morbidly obese but most people who go off of it gained the weight right back because it doesn’t change their lifestyle. It only changes their feeling of fullness.
Sadly, you don’t gain back muscle at the rate that you gained back fat. It’s very difficult, especially as your age. Worse than that is if you lost bone. Good luck getting that back at all..
Be very careful do your research before promoting something that seems like a miracle and may be for very specific cases.
In the end, it’s all insulin and insulin response. Becoming insulin resistant overtime to the massive amounts of simple carbohydrates we eat.
Good article, but I don’t agree with the premise that this should become massively widespread without serious critical analysis of the outcomes.
This is so American. Don’t look at the root problem. Take a pill or shot. What caused the problem? Too many carbohydrates. How to fix the problem? Quit eating so many. Problem fixed medicine is your food.
its systemic ,,, there b lots of money in problems ,,, if other countries could make that much on problems , they would ….
At $50 a dose and $12B over 2 years, there is more than 1 billionaire that could fund that program while donating less than 10% of their wealth.
I have no issue with the article although I wish the government would also outlaw highly processed food. The bigger issue is that the US government isn’t rational anymore. Their policies only support the pillaging of the economy with almost no thought for the future. We are already living very close to the Rollerball (1975 version) vision except that even James Caan wouldn’t stand a chance today.
Hopefully Scott isn’t letting ai write these newsletter. Lots of “it’s not X — it’s Y.” Ai slop. But maybe he used that phrase before ai made writers lazy. Idk
Bariatric sleeve surgery is far more efficient for people with a BMI over 40 than taking GLP-1s, and in most countries it is far cheaper. It gives people long-term effectiveness and sustained weight loss: Many patients maintain a significant portion of their weight loss for 10 years or more, with average excess weight loss of 51–54% at the 10-year mark.
GLP-1s are being released in a pill form at the end of this year. I see the target market as those who want to lose 5 to 10 kilos and then really commit to keeping it off.
Bariatric sleeve surgery is generally more effective for long-term weight loss than GLP-1 medications alone. Studies show bariatric surgery leads to greater and more sustainable weight loss, significant improvements in other health conditions, and is often more cost-effective in the long run due to lower ongoing medical costs compared to lifelong medication use.
Calories are just like dollars; addiction to either leads to physical, emotional and/or mental health issues.
….and, like other forms of addiction (drugs, alcohol, sex, etc.), very, very hard to disconnect from.
It’s been stated and verified long ago that the culprit is sugar and the sugar industry. Talk to a biologist or a biochemist and they’ll tell you that sugars are in the category of simple carbohydrates and offer nothing to help one’s metabolic process. If you’re feeling fatigued, don’t have a candy bar (simple carbohydrates), instead, have a piece of fruit or raw vegetable (complex carbohydrate). Without exercise, the simple carbohydrates settle in one’s body fat more easily than complex carbohydrates.
The problem is NOT fats! Animal protein with fats in it, such as beef, pork or even fish, is healthier than a manufactured sugar product like a candy bar or Southern Style BBQ Sauce. We need the fat from animal protein to help metabolize fat soluble vitamins and to provide elasticity to our skin and our joints. Please stop the fat bashing! It’s processed sugar that is the problem!
I agree more with you than you do with yourself.
A year ago I gave up all sugar and bread. The increase in my energy was incredible. My blood is now like the finest elixir on the planet.
It’s really not that hard.
JLM
“We spend $13,000 per person, versus $6,500 in the rest of the G7.”
Who collects the difference?
That comment was meant for the general track.
We overpay our physicians (and limit our medical school access) by about 35% for pcps (now largely imigrants) and by 2-5x or more for specialties vs other industrialized countries. We overpay for our ethical drugs by about 2-3x (despite having the highest generic discounts in the world), we overpay for our hospital delivery system by about 2x vs other OECD countries and we overpay our private insurance by about 2x vs the private/public insurance in OECD countries. That is how we pay slightly over 2x what the OECD countries pay for healthcare – the excess is spread pretty equally across the industry.
I know who we pay. I pay too. My question was who collects.
This comment is for you. No one presses a gun to our heads, forcing us to eat so much sugar. I do not.
Pure White and Deadly by John Yudkin, a British professor of Nutrition, was published over 50 years ago. Its findings on sugar are clear for all to see, but were they acted on? Not effectively at all.
GLP-1’s are not really ‘weight-loss’ drugs. They’re hormones that correct metabolic imbalances, just like insulin. And one of the side effects of balancing your metabolism is that you lose weight. I’ve been taking Zepbound/Mounjaro for 2 years and dropped 60 pounds but the real benefit is that,for the first time in my life, at 75, I’m only eating what I need and my body is processing it properly. Plus a bunch of other benefits like lower A1C and blood pressure. And, as long as I can afford it(!), I’ll be taking it for ever as the metabolic benefits don’t continue without taking it.
On Scott’s point about the expense of US healthcare versus its effectiveness as compared to the G7 he seems to have missed the elephant in the room – the US healthcare system. All the intermediaries that exist in the US system – insurance companies, Pharmacy Benefit Managers and the rest – extract, not add, value. They are literally increasing the cost and adding no benefit. Maybe mention that next time?
This is entirely anecdotal, but here goes:
1/ Through various happenstances/work, etc, I’ve come across people taking ozempic, (who already had diabetes), and their diabetes/insulin levels were completely out of control and ended up in hospital. (Very dangerous) I was chatting with an EMT at one scene, and asked if this was becoming common (uncontrolled diabetic emergencies in Ozempic users), and she said she was seeing a fair bit of it. These were people in their 40s. I doubt the manufacturer is looking too hard for these issues, but apparently there are some, so be careful
2/Also heard, from lots of people who were diabetic (before Ozempic came out), that intermittent fasting is a lot easier that people think, and extremely effective in developing habits that curb appetite. IOW, might be a much safer alternative
Obesity is one of those things that many (most?) people don’t (or don’t want to) understand. It’s bad, cheap, tasty calories available and in your face in all your waking moments. It’s genetic. It’s lack of exercise (or, for some, the opportunity to exercise). It’s addictive personality. It’s screen time. It’s sedentary work life. It’s all that and more. Not everybody can use GLP-1 drugs due to personal side effects. But for those of us who can, they are, literally, life-changing. Without the buzz of food attraction (or is it addiction… I won’t get into that argument, although I have a strong opinion) everything in my life has had added clarity, and I’m not carrying around those extra 40 pounds. If you haven’t been there or adjacent, you don’t really know. If you think the answer is a re-run of “Just Say No”, you are unclear on the concept. And a request… If you have judgments about people who are obese, but you don’t know them or their circumstances, kindly STFU and keep your opinions to yourself.
Next up, fix the MBA system that focuses on consumer manipulation. Like ‘Brand Management’ course work….
Wrong solution. When there are buyers for the Brooklyn Bridge, there will be sellers. They do not need a college education. Teach consumers.
I would like to use it in pill form. I would hope that I could use it for a year or less, and lose 20 some pounds and be able to stop using it. I don’t think it would be good to use it for an extended period of time.
I just spent 1 month cycking from North to South in the USA, I’m a Brit. From Montana to Arizona every gas station and store sold 500ml cans and bottles of sodas like coke and nothing smaller.
What happened to a “ normal “ 330ml can of coke?
I also noticed that bottled warer was very scarce on the shelves, in UK which i’m not saying is ideal there is probably nearly as much choice of water as colas. In. uS water was obscure, just a few sku’s.
WTF?!? Here in Canada I’ve never seen the 500ml cans, just the usual 333ml and also the 227ml smaller ones.
This week’s post reminded me of the recent South Park movie “The End of Obesity.” Explains the whole thing in typical South Park fashion, though without as much detail on the economics. I really do feel that every healthcare provider should watch this to make sense of it all.
I wish I had done it when my doctor first recommended it. I’ve been on it for 10 months and am down about 30 pounds with no will power required (and no malice or mercy!).
Scott, regarding “RFK Jr. has called for “lifestyle” changes while cutting NIH funding” — is there really not enough educational content available on YT, etc.? Perhaps we need to reinforce healthy diet in schools vs. accepting everyone regardless of their weight? Also, do we need the government to step in to help? “fat generals”/leaders should know the impact of bad health and eating habits. It’s similar to an overweight Doctor. Do we need a government program to explain to Doctors the downside of a poor diet + lack of exercise?
Agree, 100% with your comment here Scott-
Don’t know why prof G has to always attack Trump, hegseth, and RFK – just because they speak the truth and are correct in their statements, doesn’t mean they need to be criticized because you don’t agree with them politically…
Shouldn’t people eat better food and exercise more?
Shouldn’t young kids be taught these better habits right from the start?
Shouldn’t higher ups in the military be physically fit?
These are not difficult questions to answer…
Two comments: GLP’s made me really, really sick and I tried different, ever smaller doses for a year. So there’s that.
And….I bought a bunch of Eli Lilly for just the reasons you described, held it for 6 months, lost a lot of money and sold it. Til this day, I don’t get it. I always thought it was a sure bet as well.
100%, GLP1’s appear to be the only way out of our obesity situation. Obesity is related to about 200 diseases. The downstream healthcare costs are massive.
How about just eat less garbage food, and get some steps in every day…
Drugs are not always the answer.
It’s the answer for less motivated people that want to keep eating unhealthy food and not do any exercise…
The American Heart Association just released the real obesity stats, and the feel-good 40% figure has grown to 70%! Athletech has already “weighed in”.
READ what ChatGPT said when asked why a major Fitness Industry publication would tell its readers what they don’t want to hear.
“So Athletech’s ’70 %’ isn’t a revelation; it’s positioning — getting ahead of the story before the numbers become undeniable.”
I published similar stats for years. (Read my Substack)
The question now is: will the government replace fluoride in the water supply with Semaglutide?
All puns and jokes aside, our future bodies have a solution — particularly if we embrace Hara Hachi Bun Me, as they do in Japan, where obesity is 3.8%. See 80bites.com.
“They get you addicted to sugar and salt, then hand you to the “non-health” complex for replacements, dialysis, and statins.”
No, “They” don’t get you addicted. You get yourself addicted.
And btw, once you’re on GLP-1’s, you have to stay on them to maintain the results. I’ll be eagerly awaiting Prof G’s screed on this in the coming years.
Universal Health Care. Free healthy meals K-12. Free pre-natal care. Aerobics PE K-12.
By the looks of some people I see, they aren’t struggling very hard.
Hey Scott
I have been on Ozempic (high blood sugar) for 9 months. Went from 210 Lbs to 173 Lbs, now stable at that weight. Blood sugar fixed, blood pressure fixed, sleeping fixed. So… great.
From an impact on GDP Pov… not so good. I stopped red wine (makes me feel sick at the thought); I eat way less; I only have 1 coffee (not 6).
My guess is my consumption dropped by thousands of $ a year.
For a Yorkshireman, saving all that money must be the big win. Keep on creating, Keith.